Adrenal Insufficiency
What is Adrenal Insufficiency (AI)?
What is Adrenal Insufficiency (AI)?
Adrenal insufficiency occurs when there is not enough active cortisol to maintain the body’s needs. This can be:
A. Acute: from mild to a serious immediate life-threatening shortage of cortisol (Adrenal crisis);
B. Chronic or a long-term shortage caused by damage or disease that has affected the ability of the adrenal glands to produce enough cortisol;
C. Primary: because of failure of the adrenal glands (Addison’s disease);
D. Secondary: because of failure of ACTH from the pituitary gland;
E. Tertiary: when the adrenals no longer produce cortisol after long term treatment with steroids such as cortisol/prednisone/dexamethasone.
ADRENAL INSUFFICIENCY can be life-threatening!
What does Cortisol do?
WHAT DOES CORTISOL DO?
Cortisol manages a wide range of bodily functions. It’s a key hormone in the body’s protective responses to stress – prepares the body for ‘fight or flight’ survival and is essential to sustain life.
Cortisol does this by maintaining:
– Blood sugar level for energy production.
– Salt and water balance to maintain adequate blood volume.
– Blood pressure and increasing this as needed for fight and flight.
– Immune function and suppressing inflammation in case of injury.
– Cognitive focus concentration, adjusting mood and memory.
– Sleep/wake cycle in concert with melatonin.
What controls the Production of Cortisol
WHAT CONTROLS THE PRODUCTION OF CORTISOL?
Cortisol is a steroid hormone that is made in the outer area or cortex of the adrenal glands. The body is in a constant state of alertness to balance bodily maintenance functions or to protect if the need arises with fight or flight. Cortisol has a role in balancing body fluid levels, fighting infection and producing energy.
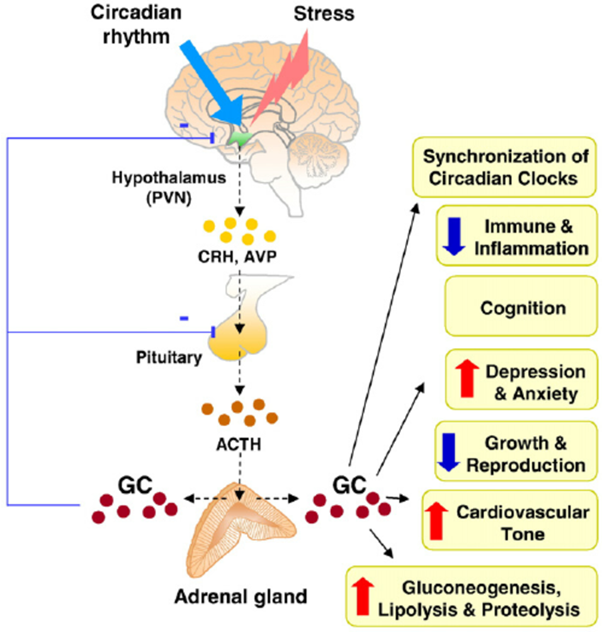
The Hypothalamus, pituitary and adrenal glands work together to keep the body balanced. Like a room thermostat that directs the heater to turn on or off accordingly to keep a set temperature, when the hypothalamus senses low cortisol levels it secretes corticotropic releasing hormone (CRH) into the pituitary. The pituitary responds by secreting Adrenocorticotropic Hormone (ACTH) that travels through the blood and attaches to receptors on the adrenal cortex. ACTH instructs the cells of the outer cortex of the adrenal glands to produce cortisol.
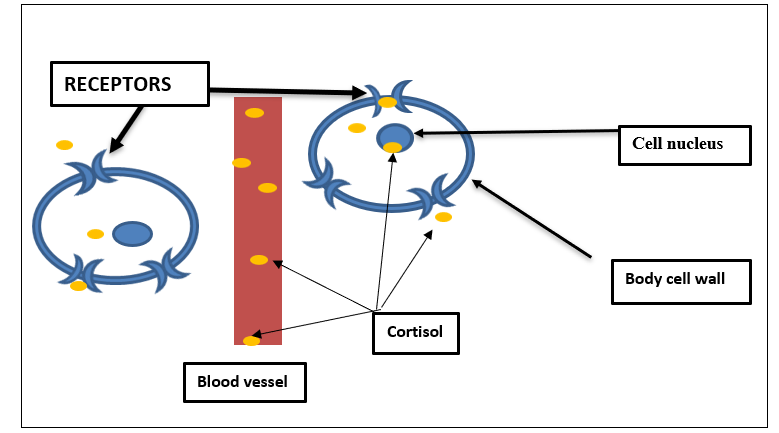
Cortisol is then released into the blood and distributed to most body tissues. It attaches to glucocorticoid receptors and is taken into the body cells to perform multiple actions. In the liver, glucose (sugar) is produced and from the pancreas insulin is produced, which helps sugar enter cells to power energy needs. In all muscle (including heart muscle), fat, carbohydrates and protein are broken down for energy. In blood vessels, cortisol manages the amount of dilation, constricting blood vessels when more blood pressure is needed. In the brain, cortisol helps to sharpen alertness, focus attention and concentration on the task at hand. When the level of cortisol in the blood is adequate to maintain all the tissue functions, this signals the hypothalamus and the pituitary to stop production of CRH and ACTH. Once the cortisol is used and the level falls, this signals the hypothalamus and pituitary to restart secretion.
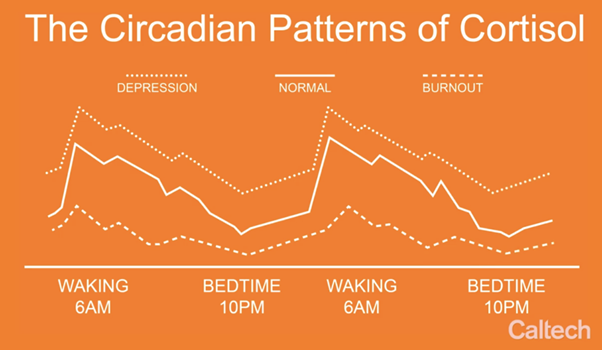
Production of cortisol follows a 24 hour ‘circadian pattern’. The highest production of CRH and ACTH is early in the morning which ‘turns on’ the production of cortisol and subsequently lowers the need for ACTH production. Cortisol provides ‘get up and go’ to start the day. During the day the ACTH remains relatively low unless there is increased stress or a need for ‘flight or fight’.
At night or at the onset of sleep, cortisol levels are usually very low in order to allow the body to rest and repair.
What happens when NOT enough Cortisol is produced?
What happens when not enough cortisol is produced?
Adrenal insufficiency (AI) occurs when not enough cortisol is produced by the adrenal glands.
AI can happen when the adrenal gland cells are unable to produce sufficient cortisol. This is known as primary adrenal insufficiency or Addison’s disease. Cortisol production requires multiple manufacturing steps in the adrenal gland. If there is an absence or a shortage of all the ingredients needed the adrenal gland cells fail to make cortisol. ACTH may continue to try to activate the process by getting higher, but the adrenal glands cannot respond.
Primary adrenal insufficiency (PAI) can occur because the tissue of the adrenal glands has been destroyed by infection or an autoimmune disease. In the latter, the body’s defense (immune) system has mistakenly attacked this tissue. PAI may also be the result of a genetic mutation or mistake in one or more steps in the process of cortisol production in the adrenal glands. This may be congenital PAI found at birth or soon after.
The key symptoms of PAI
Salt craving, salt loss, lethargy, and muscle weakness weight loss.
Secondary adrenal insufficiency (SAI) can occur when the pituitary gland fails to produce enough ACTH to stimulate the adrenal production of cortisol. This may happen after a hemorrhage in the pituitary gland, with injury, infection or as the result of a pituitary tumour with and without surgery.
Tertiary adrenal insufficiency is the result of long-term steroids given for the treatment of another disease such as cancer, rheumatoid arthritis, Crohn’s disease and more. Over time, the adrenals lose their ability to produce cortisol and become dependent on the medication being administered.
AI can also be considered Acute or Chronic. Chronic adrenal insufficiency may be well controlled on replacement doses of glucocorticoids (cortisone. dexamethasone, hydrocortisone, methylprednisolone, prednisolone).
Acute adrenal insufficiency can be a life-threatening crisis condition.
Acute Adrenal Insufficiency is most often caused by an infection, fever, illness, or injury (such as a car accident, broken leg skiing, severe emotional stress) The immediate administration of a stress dose may be indicated if symptoms are severe.
Symptoms of Adrenal Insufficiency
|
|
Symptoms of Adrenal Insufficiency
Headaches
Nausea that may progress quickly to vomiting
Dizziness because of low blood pressure, and may lead to fainting
Abdominal pain and diarrhea
Craving for salty foods because of low blood sodium (salt)
Hypoglycemia, or low blood sugar levels
Joint pain and weakness
Fatigue
Confusion, difficulty thinking when sodium (salt) levels are very low.
Chronic fatigue
Loss of appetite that leads to weight loss
irritability and depression
irregular or no menstrual periods
loss of interest in sex
Muscle weakness
What Tests Diagnose Adrenal Insufficiency
What Tests Diagnose Adrenal Insufficiency?
Cortisol molecules that are ‘free’ or not attached to other molecules in the blood may be sampled with a random blood draw, in the early morning when the highest levels are expected. Low levels in the early morning suggest insufficiency but levels may be difficult to interpret and require further testing to diagnose adrenal insufficiency.
A 24 hour urine for free cortisol and morning saliva levels of cortisol can be collected and measured against a normal standard cortisol excretion.
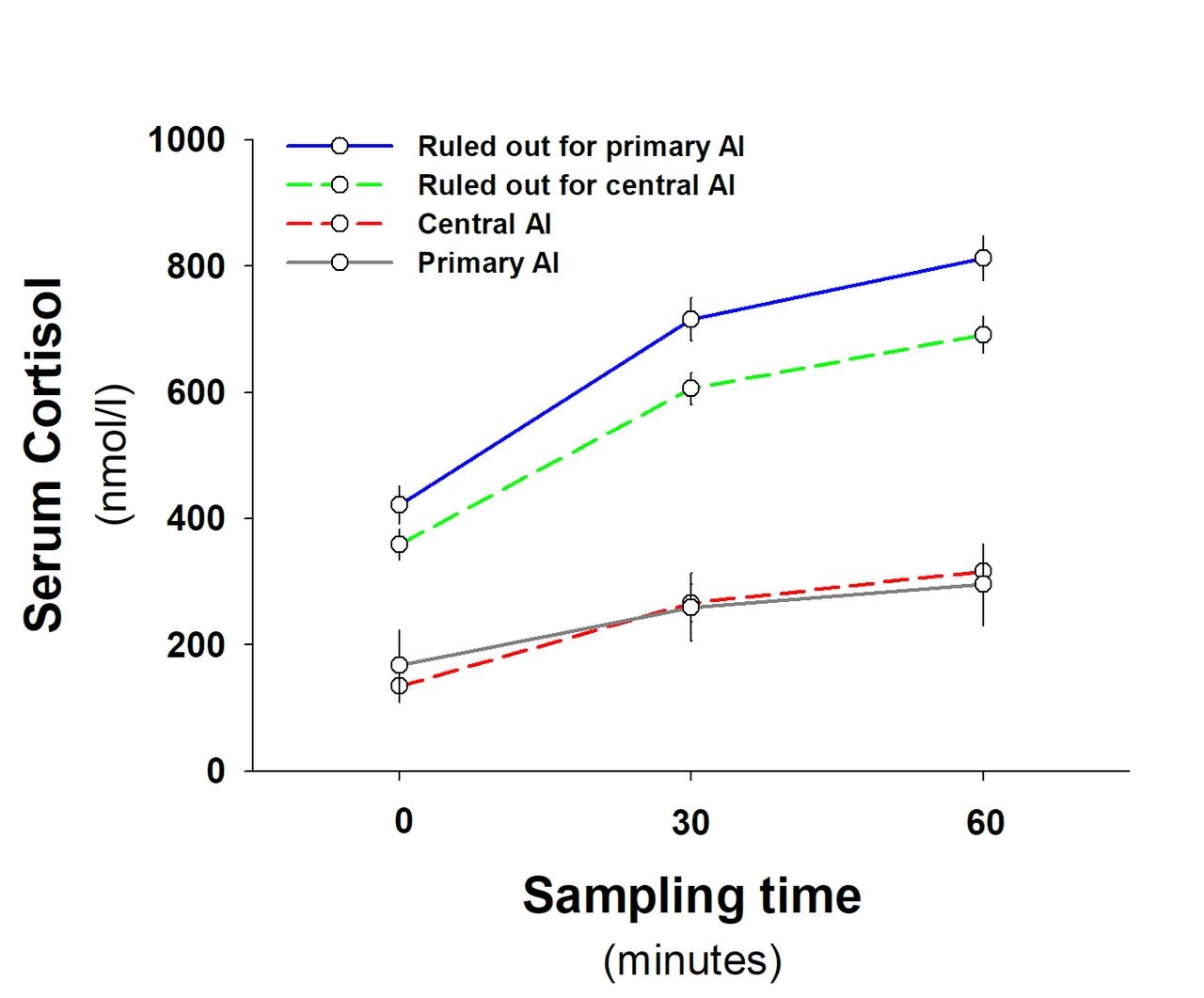
Other tests referred to as dynamic tests are usually a more accurate means of diagnosing AI. These tests stimulate the adrenal glands to produce cortisol. The ‘gold standard’ test (test considered the most reliable), is an insulin tolerance test (ITT). However, this is labor and time intensive and not considered appropriate for patients over the age of 55, with seizure disorder or heart disease. Therefore, a cortrosyn stimulation test or a metyrapone stimulation test are used. Currently, the former is more commonly used.
Insulin tolerance test involves the administration of insulin to induce hypoglycaemia. This stress causes the hypothalamus to secrete CRH, the pituitary ACTH and stimulates the adrenals to produce cortisol. Cortrosyn is a synthetic form of ACTH which stimulates the adrenals directly to produce cortisol. Metyrapone test is used to determine the production of ACTH from the pituitary or for secondary adrenal insufficiency. Metyrapone lowers the cortisol levels, signaling the hypothalamus to produce CRH and subsequently the pituitary to produce ACTH. If ACTH remains low, along with cortisol, then secondary adrenal insufficiency is diagnosed.
How can I avoid ADRENAL CRISIS / Acute Adrenal Insufficiency?
HOW CAN I AVOID ADRENAL CRISIS / Acute Adrenal Insufficiency?
Know the symptoms of AI
Be prepared – keep extra of your regular medication (typically hydrocortisone) quickly available at home, in your place of work, in your car, in your wallet. Wear medical alert jewelry, carry a medical alert card to indicate you have adrenal insufficiency with instructions to administer a ‘stress’ dose of steroids if you are unable to do so yourself.
Take a ‘STRESS DOSE’:
- Double/triple regular dose (hydrocortisone, prednisone, dexamethasone etc),
- at the onset of symptoms:
e.g. fever or illness, extreme stress, injury or prior to a medical procedure. - Continue at least 4 days.
- Contact your Endocrine Team!
Learn how to increase your dose with unusual physical activity or other stressful activities such as prior to an exam, a busy social event, or an air flight.
Surgery and the onset of labour during pregnancy are special circumstances and an increased dose of steroid is needed.
Talk with your medical team for recommendations.
If symptoms are getting worse, give an emergency injection of Solu-Cortef into a muscle.
Make sure your family and friends can also administer this injection if you are not able to do so.
Fast action can save your life!
WHAT TO DO IF I HAVE AN ADRENAL CRISIS?
WHAT DO I DO IF I HAVE an ADRENAL CRISIS?
Administer an intramuscular injection of Solu-Cortef 100mg
- Open the package containing the Solu-Cortef, the syringe with needle, twist needle to tighten
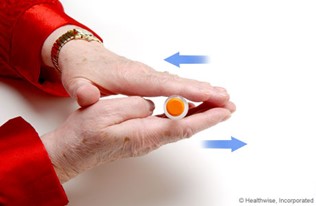
Keeping the vial on a flat surface, push down the rubber stopper on top of the vial of Solu-Cortef:

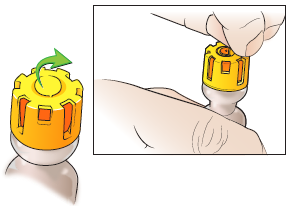
2. Roll the vial between your hands until the powder in the bottom of the vial is fully dissolved (clear solution; no shaking, no bubbles).
3. Remove the small round plastic disc in the middle of the vial and clean the top with an alcohol swab (if not available, please take next step).
4. Insert the needle into the orange rubber stopper in the middle of the top of the vial and turn the vial upside down.
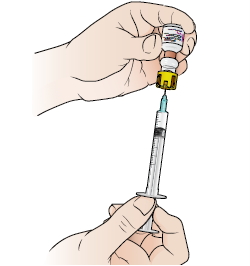
5. Withdraw all the fluid from the vial by pulling the bottom of the plunger on the barrel of the syringe.
6. Remove any air from syringe by tapping the barrel of the syringe then push out any air bubbles by pushing up a little on the plunger of the syringe.
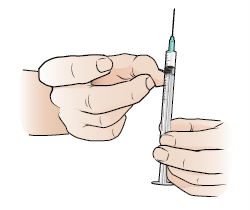
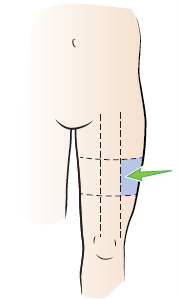
7. Chose and injection site on the side of the thigh as pictured and clean with an alcohol swab.
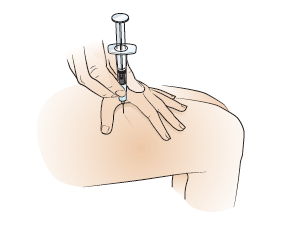
8. Hold the syringe like a pencil and stab the needle into the cleaned site at a 90degree angle.
Most of the needle should be below the skin.
Push slowly down on the plunger to administer all the fluid in the syringe.
Hold to the count of 10 then remove the syringe.
9. Seek emergency medical care to ensure the acute episode has resolved and to determine the cause of the adrenal insufficiency.
DON’T WAIT- INJECT. This may save a life … your life!
Abbreviations
Abbreviations
ACTH Adrenocorticotropic hormone
AI Adrenal insufficiency
PAI Primary adrenal insufficiency
SAI Secondary adrenal insufficiency
CRH Corticotropin releasing hormone
References
References
Braun TP, Marks DL. The regulation of muscle mass by endogenous glucocorticoids. Front Physiol. 2015;6:12. Published 2015 Feb 3. doi:10.3389/fphys.2015.00012
Hirotsu C, Tufik S, Andersen ML. Interactions between sleep, stress, and metabolism: From physiological to pathological conditions. Sleep Sci. 2015;8(3):143-152. doi:10.1016/j.slsci.2015.09.002
Li D, Genere N, Behnken E, et al. Determinants of Self-reported Health Outcomes in Adrenal Insufficiency: A Multisite Survey Study. J Clin Endocrinol Metab. 2021;106(3):e1408-e1419. doi:10.1210/clinem/dgaa668
Dineen R, Thompson CJ, Sherlock M. Adrenal crisis: prevention and management in adult patients. Therapeutic Advances in Endocrinology and Metabolism. 2019;10. doi:10.1177/2042018819848218
Oprea A, Bonnet NCG, Pollé O, Lysy PA. Novel insights into glucocorticoid replacement therapy for pediatric and adult adrenal insufficiency. Therapeutic Advances in Endocrinology and Metabolism. 2019;10. doi:10.1177/2042018818821294
Ospina NS, Nofal AA, Bancos I, Javed A, Benkhadra K, Kapoor E, Lteif AN, Natt N, Murad MH. ACTH Stimulation Tests for the Diagnosis of Adrenal Insufficiency: Systematic Review and Meta-Analysis, The Journal of Clinical Endocrinology & Metabolism, Volume 101, Issue 2, 1 February 2016, Pages 427–434, https://doi.org/10.1210/jc.2015-1700
Author:
Chris Yedinak DNP, FNP
Associate Professor
Oregon Health & Sciences University Portland. OR. USA
Last updated: November 2022